Henrique Augusto Lino 1, André Mannato 2, Diego Cardoso Fragoso 3, Henrique Bortot Zuppani 4
Abstracto
A 12-year-old male presented proptosis of the right eye, nasal obstruction, and headaches for a month. The computed tomography (CT) showed an expanding and insufflating lesion with heterogeneous attenuation coefficients, mostly hyperattenuating, located at the right nasal cavity. The histopathological examination concluded the tumor as a cemento-ossifying fibroma. Afterward, the lesion was enucleated.Dados do caso
Mal, 12 anos.
Palavras chaves
Cementoma, Tumores Odontogênicos, Fibroma, Fibroma Ossificante.
Histórico Clínico
A 12-year-old male presented proptosis of the right eye, followed by nasal obstruction and headache for about a month. The rhinoscopy showed a bony-consistency lesion posteriorly to the right middle turbinate. It was bulging the local structures and decreasing the caliber of the air column. The patient underwent enucleation.
Achados Radiológicos
The CT scout reveals an expanding and insufflating heterogeneous lesion with circumscribed and hyperdense borders projecting over the orbital and nasal topography (Figure 1). The CT showed a predominant hyperdense oval-shaped expanding bone lesion with some insufflating characteristics and circumscribed borders, measuring about 5,3 x 4,1 x 3,6 cm. It was centralized at the right lamina papyracea with an extension to the homolateral sphenoid sinus (Figures 2 and 3). The lesion determined bone remodeling and expansive effect over the adjacent structures, which was mainly characterized by the extrinsic compression of the orbital components (Figures 4 and 5). The most compromised eye structures were the ones near the orbital apex of the right side with lateral displacement of the extraconal fat, inferior and medial rectus muscles of the eye and the optical nerve.
Discussão
The cemento-ossifying fibroma (COF) is a benign mesenchymal odontogenic tumor, according to the 2017 World Health Organisation’s classification [1]. The COF is rare neoplasia, often occurring on female patients between the third and fourth decade of life. The most commonplace of involvement is the mandible in about 70% of the cases [2]. The COF’s etiology is unknown, but it has been supposed that local trauma may trigger its development. The lesion usually arises from the adjacent dental elements of the mandible and the maxilla. The lesion is composed of pluripotent cells from the mesenchymal tissue of the periodontal ligament with the capability to differentiate into fibrous tissue, cemento, bones, and mixed-composition tissues [3,4]. The radiological aspect of the COF is represented by a mixed radiolucent and radiopaque lesion, with multiple compartments, a definite capsule, circumscribed borders, and sclerotic margins. As the tumor maturates, it becomes radiopaque [5]. The lesion has two types: adult and juvenile [1]. The first one affects women between the third and fourth decade of life, usually appearing as an incidental finding on an asymptomatic patient [6]; the latter ones manifest on young male patients, generally younger than 15 years old, with more aggressive and expansive behavior. In some cases, it may also behave as a destructive lesion, and it may compress adjacent structures. The juvenile type has the highest recurrence rate (roughly 30-58%) [2], as the presented case. COF’s management depends upon some factors, like location and dimensions. The small tumors might be enucleated or curetted. The larger and aggressive lesions, on the other hand, must be resected with wide resection margins. Eventually, this latter group of patients may also benefit from chemotherapy with alfa-interferon or subcutaneous calcitonin. Radiotherapy is avoided because it increases the malignancy rates of the lesion. Regardless of the treatment, the COF should be monitored in order to detect recurrences [2].
Lista de Diferenciais
Diagnóstico
Aprendizado
We report a case of a patient with a juvenile type of cemento-ossifying fibroma with fast progression and expansive behavior determining symptoms. The juvenile COF (the aggressive variant) has the highest rates of recurrence. Thus, its recognition is relevant in order to plan the proper management.
Referências
[1] Bala TK, Soni S, Dayal P, Ghosh I. Cemento-ossifying fibroma of the mandible: A clinicopathological report. Saudi Med J. 2017;38(5):541–5.
[2] Aburas S, Bandura P, Al- Ibraheem A, Berger S, Meier M, Turhani D. A large maxillary cemento-ossifying fibroma superimposed with solitary bone cyst documented over 18 years: A case report. Int J Surg Case Rep [Internet]. 2020;68:257–62. Available from: https://doi.org/10.1016/j.ijscr.2020.03.011
[3] Singhal A, Singhal P, Ram R. Cemento-ossifying fibroma. Contemp Clin Dent. 2012;3(1):83.
[4] Chang HJ, Donahue JE, Sciandra KT, Evangelista PT. Best cases from the AFIP juvenile ossifying fibroma of the calvaria. Radiographics. 2009;29(4):1195–9.
[5] Dunfee BL, Sakai O, Pistey R, Gohel A. Radiologic and Pathologic Characteristics of Benign and Malignant Lesions of the Mandible. RadioGraphics [Internet]. 2006 Nov 1;26(6):1751–68. Available from: https://doi.org/10.1148/rg.266055189
[6] Toledano-Serrabona J, Núñez-Urrutia S, Vegas-Bustamante E, Sánchez-Torres A, Gay-Escoda C. Florid cemento-osseous dysplasia: Report of 2 cases. J Clin Exp Dent. 2018;10(11):e1145–8.
Imagens
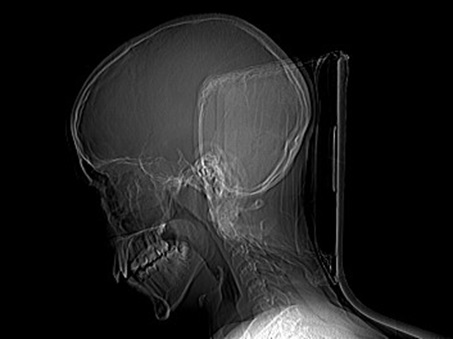
CT scout reveals an expanding and insufflating heterogeneous lesion with circumscribed and hyperdense borders projecting over the orbital and nasal topography (arrows).
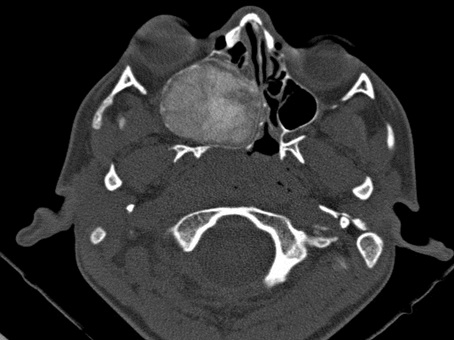
An axial CT (bone window) image shows and expanding and insufflating heterogeneous mass with an oval shape and defined borders. Its content consists of mixed attenuation of bony and soft tissues. The lamina papyracea is the center of the lesion. Medially it displaces the nasal septa to the left as well the nasal turbinates. Laterally the tumor extends to the right maxillary antrum. Anteriorly it reduces the space of the right orbit, mainly its apical segment, and it displaces the eye.

A sagittal CT (bone window) image shows the lesion is extending to the right anterior clinoid process, the sphenoid plane, and the floor of the sella turcica. Inferiorly it touches the hard palate.
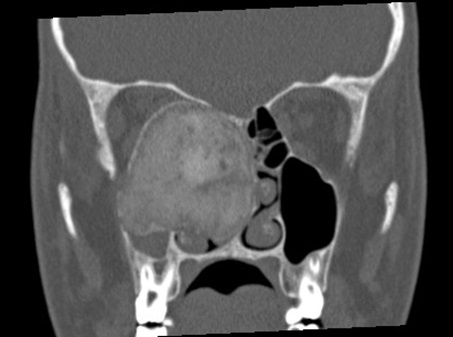
A coronal CT (bone window) image reveals the mass occupies most of the right maxillary antrum extending to its posterolateral wall. Medially it touches and displaces the bony portion of the nasal septum. The right-sided ostiomeatal and sphenoethmoidal recess are obliterated.

Frontal view of a three-dimensional CT reconstruction demonstrates a bone mass extending to the floor and medial wall of the right orbit (arrows).
Artículo recibido en viernes, 15 de mayo de 2020
Artículo aceptado el viernes, 19 de junio de 2020
 Todos los artículos científicos publicados en brad.org.br están bajo una licencia Creative Commons.
Todos los artículos científicos publicados en brad.org.br están bajo una licencia Creative Commons.
 Portugués PDF
Portugués PDF
 Impresión
Impresión
 Enviar este artículo por correo electrónico
Enviar este artículo por correo electrónico
 Cómo citar este artículo
Cómo citar este artículo
 Enviar un comentario
Enviar un comentario
 Mendeley
Mendeley
 Pocket
Pocket